Osteoporosis
Bone Metabolism
Osteoporosis is a slowly progressive loss of bone mass with age. It is a normal part of the ageing process but may be accelerated in abnormal situations. Generally, Osteoporosis develops slowly without obvious symptoms. Eventually, however, stature may decrease, and the spine may curve to create a fixed hunched alignment. The most worrisome effect of osteoporosis is the increased risk of fracture with progression. More than 25 million Americans are affected by osteoporosis and nearly 1.3 million bone fractures occur per year as a direct consequence. These are the most serious consequences of osteoporosis, with wrist, spine and hip fractures most common. They contribute to significant pain, disability, and a large expense. The causes of Osteoporosis are not fully understood. The quantity of bone mass slowly declines with age in both men and women beginning about age 35. This bone loss is accelerated with the onset of menopause, accounting for a fracture rate in women more than double that in men.
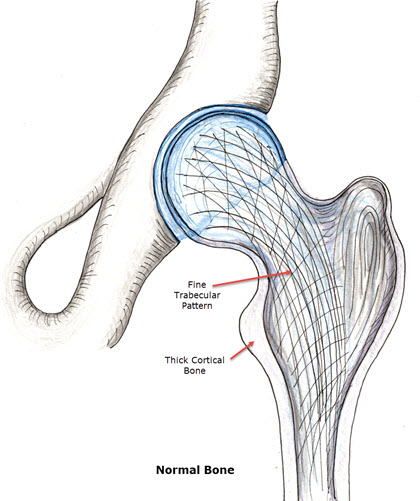
Bone is not a static material. Instead, it is constantly laid down and removed at the same time. In one year, the bone you have today will be completely replaced. Because of this, minor alterations in bone metabolism may lead over years, to severe bone loss and the risk of fracture. As bone remodels with age, a young small bone with thick cortical walls develops into a large diameter bone with thin cortical walls and overall lower strength. The bone quality is identical, but the overall quantity is reduced and spread over a greater area. The same metabolic turnover of bone allows us to heal fractures. To understand this, one must have a basic appreciation for bone metabolism. Bone is made of a collagen matrix (protein lattice) with calcium-phosphate crystals deposited in a special pattern. Too much calcium and phosphate in the body fluids may result in bone formation in abnormal locations. Too little of either or both may result in an abnormal or weakened bone. The body has complex mechanisms to combat abnormalities in calcium especially. This is because calcium in the blood must be kept within a very narrow range for muscle nerves and the heart to function. The bone is used as a huge calcium reserve, and during times of need, calcium may be mobilized from bone to maintain the blood concentration. Inadequate dietary intake of calcium leads to an imbalance in bone formation in favor of bone destruction and eventual Osteoporosis (weak bone). Vitamin D, generally formed when sunlight shines on the skin, is a major factor in the absorption of calcium from the intestine, and control of calcium and phosphate balance by the kidneys. Inadequate Vitamin D, like calcium intake, may result in weakened bones. Several hormonal mechanisms control normal calcium and phosphorus balance. thyroid and parathyroid functions are necessary for normal balance. Bone also responds to loading by creating more bone. We know that this serves to minimize fracture risk and increase the healing rate of existing fractures when load against gravity is applied to the skeleton. This accounts for the protective effect of exercise like walking or running, while astronauts in space are at risk of bone loss secondary to weightlessness.
Fracture Risk
The risk of fracture is based on normal individuals hereditary factors, dietary factors, and drug use. Fair-skinned women are at high risk. So are those who smoke, have poor dietary habits or need to take most anti-convulsant medications. The accurate assessment of bone mass may be made by a special X-ray exam. Dual X-ray diffraction is the most sensitive and reproducible method for assessment of bone mass. When performed, bone mass is compared to people of the same age and sex and reported as significantly below or not below the normal for that age.
Treatment of Osteoporosis 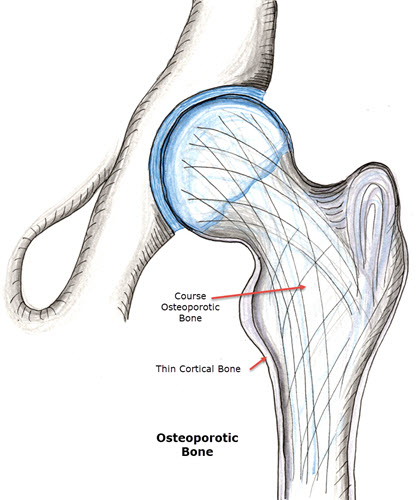
Orthopedic Surgeons are often keyed into Osteoporosis because this affects the risk of fractures which we treat. The most simple and effective treatments for Osteoporosis have already been discussed. Adequate calcium intake is simple and inexpensive with the use of calcium carbonate antacid taken daily. This is easily broken down in stomach acid and easily absorbed. Oyster shell calcium may be “natural,” but little may be absorbed. Aluminium-containing antacids should be avoided in excess, because they may actually have an adverse effect on bone mass. Normal dietary sources of calcium occur in leafy green vegetables, whole grains, and milk products. Excess calcium in the diet may cause constipation and in unusual circumstances may cause kidney stones. If you have a history of kidney stones, it is important to find out what they were made of. You should consult your urologist or general medical doctor for this information. Estrogen in normal doses has been found in women to be highly protective against Osteoporosis after menopause. This occurs because the sudden decline in estrogen results in an accelerated drop in bone density which may be halted. With estrogen, bone density is maintained in a similar course to that of a man. Estrogen has side effects and dangers. In normal doses, it is felt to have a very low risk of encouraging blood clot formation in the legs. A severe family history of breast cancer (mother and/or sister) is a contraindication to its use even with normal low doses in combination with progesterone. You should discuss the risks and benefits of estrogen treatment with your Gynecologist and plan on regular yearly visits prior to starting on estrogen therapy. Monthly self-breast exams should be performed as a routine screening even if estrogen is not used. Exercise is also very protective of Osteoporosis. Although swimming and bicycling are an excellent exercise for cardiovascular fitness, loading the body against the force of gravity is more effective in maintaining bone mass. Walking or jogging is, therefore, excellent exercise to maintain the bone mass. With more severe forms of osteoporosis, other treatments are sometimes utilized. This occurs when severe bone loss is noted with testing, or multiple risk factors are present and traditional methods of maintaining bone mass have been ineffective, or there is a history of prior fracture with known osteoporosis. Nasal calcitonin spray has been approved by the FDA for use with recalcitrant Osteoporosis. This is a hormone which tells the body to lay down bone. Its human form normally provides minor influence on the control of bone deposition. Diphosphonates are also available which help encourage bone deposition over breakdown. Newer forms of these have become simple to use and more predictable than their predecessors in the outcome. These have been shown to be capable of increasing bone mass instead of only slowing the progressive loss Osteoporosis. These too should be used primarily when traditional methods of treatment fail or are contraindicated.
Summary
In summary, Osteoporosis is a silent part of the aging process, whose consequences may be devastating. Normal diet and exercise help to slow its progression and some diseases may accelerate its onset. Treatment is dependent on multiple factors which are patient dependent. Please consult your doctor for further information.
Sports Medicine and Orthopaedics, East Providence Rhode Island